This pipeline uses various statistical tests to identify miRs whose expression levels correlated to selected clinical features.
Testing the association between 550 miRs and 8 clinical features across 150 samples, statistically thresholded by Q value < 0.05, 2 clinical features related to at least one miRs.
-
1 miR correlated to 'Time to Death'.
-
HSA-MIR-570
-
3 miRs correlated to 'PATHOLOGY.N.STAGE'.
-
HSA-MIR-29B-1 , HSA-MIR-200C , HSA-MIR-29B-2
-
No miRs correlated to 'AGE', 'NEOPLASM.DISEASESTAGE', 'PATHOLOGY.T.STAGE', 'PATHOLOGY.M.STAGE', 'GENDER', and 'COMPLETENESS.OF.RESECTION'.
Complete statistical result table is provided in Supplement Table 1
Table 1. Get Full Table This table shows the clinical features, statistical methods used, and the number of miRs that are significantly associated with each clinical feature at Q value < 0.05.
| Clinical feature | Statistical test | Significant miRs | Associated with | Associated with | ||
|---|---|---|---|---|---|---|
| Time to Death | Cox regression test | N=1 | shorter survival | N=1 | longer survival | N=0 |
| AGE | Spearman correlation test | N=0 | ||||
| NEOPLASM DISEASESTAGE | ANOVA test | N=0 | ||||
| PATHOLOGY T STAGE | Spearman correlation test | N=0 | ||||
| PATHOLOGY N STAGE | t test | N=3 | class1 | N=2 | class0 | N=1 |
| PATHOLOGY M STAGE | ANOVA test | N=0 | ||||
| GENDER | t test | N=0 | ||||
| COMPLETENESS OF RESECTION | ANOVA test | N=0 |
Table S1. Basic characteristics of clinical feature: 'Time to Death'
| Time to Death | Duration (Months) | 0-113 (median=13.9) |
| censored | N = 86 | |
| death | N = 61 | |
| Significant markers | N = 1 | |
| associated with shorter survival | 1 | |
| associated with longer survival | 0 |
Table S2. Get Full Table List of one miR significantly associated with 'Time to Death' by Cox regression test
| HazardRatio | Wald_P | Q | C_index | |
|---|---|---|---|---|
| HSA-MIR-570 | 1.63 | 8.376e-05 | 0.046 | 0.609 |
Figure S1. Get High-res Image As an example, this figure shows the association of HSA-MIR-570 to 'Time to Death'. four curves present the cumulative survival rates of 4 quartile subsets of patients. P value = 8.38e-05 with univariate Cox regression analysis using continuous log-2 expression values.
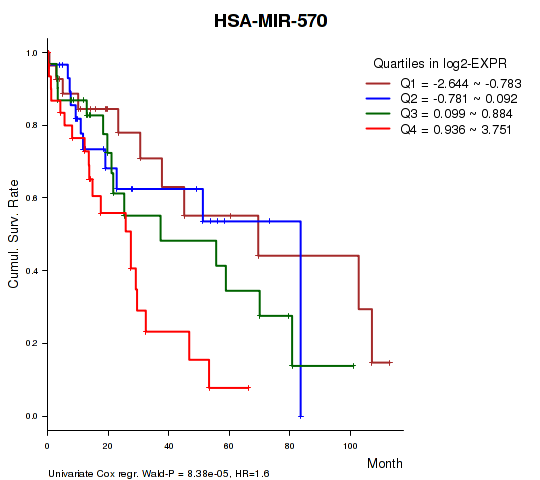
Table S3. Basic characteristics of clinical feature: 'AGE'
| AGE | Mean (SD) | 61.26 (14) |
| Significant markers | N = 0 |
Table S4. Basic characteristics of clinical feature: 'NEOPLASM.DISEASESTAGE'
| NEOPLASM.DISEASESTAGE | Labels | N |
| STAGE I | 56 | |
| STAGE II | 35 | |
| STAGE III | 2 | |
| STAGE IIIA | 33 | |
| STAGE IIIB | 4 | |
| STAGE IIIC | 6 | |
| STAGE IV | 1 | |
| STAGE IVA | 1 | |
| STAGE IVB | 2 | |
| Significant markers | N = 0 |
Table S5. Basic characteristics of clinical feature: 'PATHOLOGY.T.STAGE'
| PATHOLOGY.T.STAGE | Mean (SD) | 2.01 (0.96) |
| N | ||
| 1 | 59 | |
| 2 | 39 | |
| 3 | 43 | |
| 4 | 9 | |
| Significant markers | N = 0 |
Table S6. Basic characteristics of clinical feature: 'PATHOLOGY.N.STAGE'
| PATHOLOGY.N.STAGE | Labels | N |
| class0 | 98 | |
| class1 | 3 | |
| Significant markers | N = 3 | |
| Higher in class1 | 2 | |
| Higher in class0 | 1 |
Table S7. Get Full Table List of 3 miRs differentially expressed by 'PATHOLOGY.N.STAGE'
| T(pos if higher in 'class1') | ttestP | Q | AUC | |
|---|---|---|---|---|
| HSA-MIR-29B-1 | 5.63 | 2.543e-07 | 9.23e-05 | 0.7143 |
| HSA-MIR-200C | -4.84 | 1.374e-05 | 0.00497 | 0.7075 |
| HSA-MIR-29B-2 | 4.66 | 5.921e-05 | 0.0214 | 0.6905 |
Figure S2. Get High-res Image As an example, this figure shows the association of HSA-MIR-29B-1 to 'PATHOLOGY.N.STAGE'. P value = 2.54e-07 with T-test analysis.
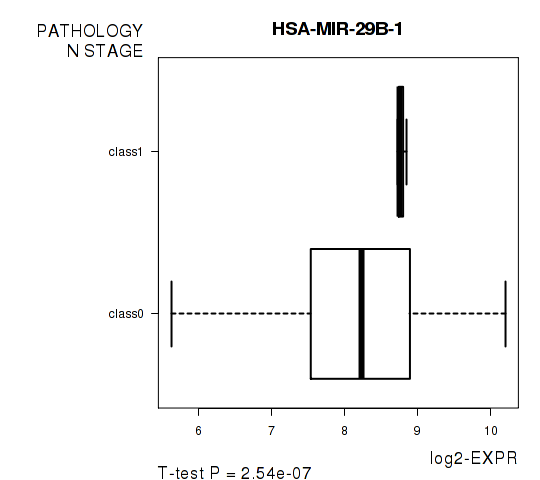
Table S8. Basic characteristics of clinical feature: 'PATHOLOGY.M.STAGE'
| PATHOLOGY.M.STAGE | Labels | N |
| M0 | 118 | |
| M1 | 3 | |
| MX | 29 | |
| Significant markers | N = 0 |
Table S9. Basic characteristics of clinical feature: 'GENDER'
| GENDER | Labels | N |
| FEMALE | 58 | |
| MALE | 92 | |
| Significant markers | N = 0 |
-
Expresson data file = LIHC-TP.miRseq_RPKM_log2.txt
-
Clinical data file = LIHC-TP.merged_data.txt
-
Number of patients = 150
-
Number of miRs = 550
-
Number of clinical features = 8
For survival clinical features, Wald's test in univariate Cox regression analysis with proportional hazards model (Andersen and Gill 1982) was used to estimate the P values using the 'coxph' function in R. Kaplan-Meier survival curves were plot using the four quartile subgroups of patients based on expression levels
For continuous numerical clinical features, Spearman's rank correlation coefficients (Spearman 1904) and two-tailed P values were estimated using 'cor.test' function in R
For multi-class clinical features (ordinal or nominal), one-way analysis of variance (Howell 2002) was applied to compare the log2-expression levels between different clinical classes using 'anova' function in R
For two-class clinical features, two-tailed Student's t test with unequal variance (Lehmann and Romano 2005) was applied to compare the log2-expression levels between the two clinical classes using 't.test' function in R
For multiple hypothesis correction, Q value is the False Discovery Rate (FDR) analogue of the P value (Benjamini and Hochberg 1995), defined as the minimum FDR at which the test may be called significant. We used the 'Benjamini and Hochberg' method of 'p.adjust' function in R to convert P values into Q values.
In addition to the links below, the full results of the analysis summarized in this report can also be downloaded programmatically using firehose_get, or interactively from either the Broad GDAC website or TCGA Data Coordination Center Portal.